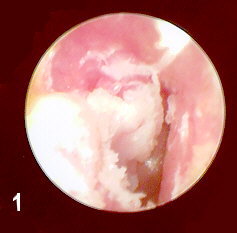
Figure 1 shows the large papilloma superficially covered by granulation tissue.
The patient is a 57 year old man with a history of a frontal angioblastic meningioma which was partially removed in 1993. His chief complaint at the time of his initial examination to the ENT Department in October 1997 was a 6 month history of a plugged sensation in his RE with some discomfort. The physical exam showed a thickening of the surface epithelium in the posterosuperior quadrant of the R TM giving a papillary appearance. The area could not be removed or separated from the substance of the TM and it did not extend into the middle ear. The tympanum was air-containing and the TM was intact.
The area was biopsied revealing a benign papillary neoplasm. The hearing was tested showing a moderate/severe high frequency SNHL with Type A tympanograms but absent ipsilateral reflex in the RE. The ear was anesthetized and the thickened area on the lateral surface of the TM was cauterized superficially with silver nitrate. The patient returned in 1 month at which time the physical exam revealed only a somewhat thickened and sclerotic posterosuperior quadrant of the TM.
Since his initial visit the patient was diagnosed with a recurrence of his benign brain tumor and had developed left hemiparesis. It was not felt that the papillary lesion was related to his brain tumor and he was instructed to return in 6 months to recheck his ear.
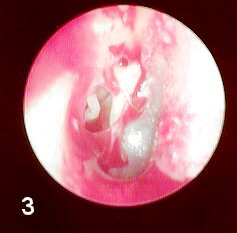
When returning in May 1998, the patient had undergone a right frontal craniotomy for a recurrent meningioma in the parasagittal area. Physical exam now revealed a large mass of granulation tissue which when partially removed showed a large papillary excrescence covering the posterosuperior 1/3 to 1/2 of the TM and now involved the medial posterosuperior ear canal skin.
Because of its recurrence and expanding nature it was decided to excise the lesion and repair the TM defect. The preoperative diagnosis was squamous papilloma but verrucous carcinoma and other infectious causes were also considered. The pathology report revealed hypertrophic reactive keratosis with acute and chronic inflammation.